Discussion
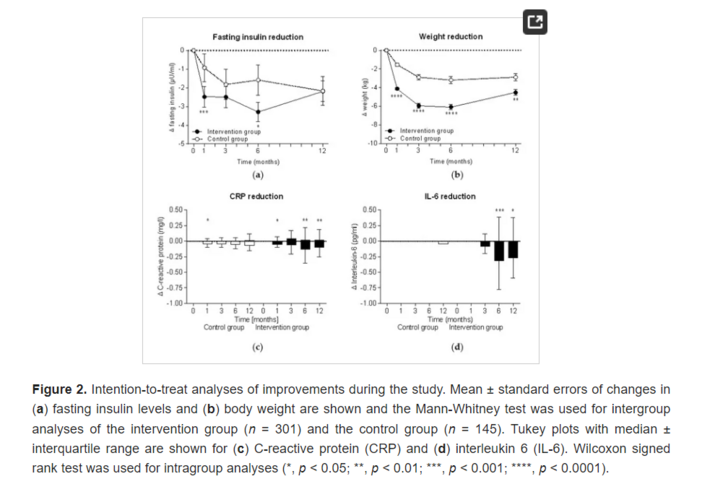
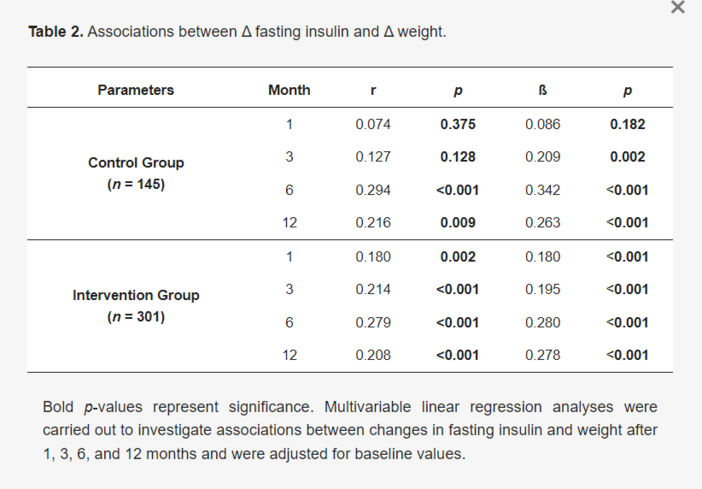
The international multicentre randomised controlled ACOORH trial demonstrated the superiority of a lifestyle intervention accompanied by a dietary change of a high-protein, low-glycaemic meal replacement compared to a control lifestyle intervention alone. Consequently, this superiority led to a greater reduction in fasting insulin levels. Furthermore, the insulin reduction correlated with the achieved weight reduction and was accompanied by improvements in inflammation markers. Participants who prematurely ended meal replacement still achieved insulin and weight improvements comparable to the control group. After the end of the intervention, both insulin levels and weight increased again but remained significantly below baseline levels.
In this subanalysis of the ACOORH trial, we primarily focused on fasting insulin as insulin not only mediates glucose uptake from the blood into the cells but also has further physiological regulatory functions. For example, insulin inhibits lipolysis at a much lower concentration than it is needed for glucose uptake [1]. By using a microdialysis technique in combination with a three-step hyperinsulinaemic glucose clamp, Jacob et al. [2] demonstrated in nineteen lean, healthy subjects that low physiological concentrations of insulin are able to inhibit lipolysis in muscle up to nearly 50% and in adipose tissue up to 75%. Thus, every insulin-releasing carbohydrate consumption might be able to slow down or even completely block lipolysis in the human body. To what degree the lipolysis is inhibited depends on the BMI. When lean people (BMI < 25 kg/m2) consumed 75 g glucose, they show only a small and short-term increase in insulin [15]. However, when people with obesity (BMI > 30 kg/m2) ingested the same amount of glucose, their insulin levels rose for hours. In fact, in participants with obesity, insulin levels were already increased in the fasting state, rose nearly twice as high after glucose consumption, and remained elevated for nearly one hour longer compared to lean individuals, resulting in an inhibition of lipolysis. When obese people consumed carbohydrate-containing meals and snacks throughout the day, the inhibitory activity of insulin on lipolysis would explain why losing weight is hardly achievable in the obese state. If obese people want to reduce weight, the first aim should be to lower their insulin levels [16,17]. Therefore, in the first phase of a diary intervention it is necessary to strictly reduce or nearly eliminate carbohydrate intake [18,19]. Furthermore, food intake needs to be reduced to a maximum of three meals per day so that insulin levels can decrease between each meal and lipolysis can be activated. Meal frequency is a controversial topic, however, the evidence in favour of a lower meal frequency was demonstrated in a recently published review [20]. Reduced meal frequency with 2–3 meals per day and regular fasting periods were shown to provide physiological benefits [21,22]. Analyses of isocaloric diets of either two or six meals per day on energy expenditure, measured in a metabolic chamber, showed a significantly higher energy expenditure at night with a two-meal diet [23]. Thus, we instructed our participants to reduce their carbohydrate intake and to eat no more than three meals per day. Participants who achieved the greatest success in losing weight were those who lowered their insulin levels the most. Therefore, measuring insulin levels could possibly be used in the future to monitor the degree of compliance with the carbohydrate restriction.
It is well known that metabolic disorders with elevated insulin levels, such as obesity, metabolic syndrome, and type-2-diabetes, are associated with and accompanied by chronic subclinical inflammation. Thus, insulin is also thought to be involved in regulating the activation status of immune cells. Normally, naive T cells gain energy by oxidation of fatty acids [4]. However, their signal to become activated is conveyed by glucose admission and a switch to aerobic glycolysis [5,24]. Activation with lipopolysaccharide (LPS) also leads to the use of glycolysis in classic proinflammatory macrophages and dendritic cells [25,26]. Another example are IL-4-induced alternatively activated macrophages, which help to suppress inflammatory signals as they become down regulated in hyperinsulinaemia and obesity [27,28,29]. As glycolysis is mainly found in inflammatory and rapidly proliferating immune cells, and in contrast long-living and anti-inflammatory cells are related to β-oxidation, it can be concluded that key enzymes and metabolic programs can instruct immune cells to carry out proinflammatory or anti-inflammatory functions. This relation could explain why increased inflammatory reactions are observed in the context of overeating with a large proportion of carbohydrates. An increased fat metabolism for immune functions, on the other hand, indicates a pronounced anti-inflammatory effect.
Various studies, in which carbohydrate restriction and intermittent fasting were part of the intervention, not only showed a significant reduction in body weight in participants who were overweight but also a concomitant decrease in the concentration of inflammatory markers in the blood [30,31,32]. Missing insulin signalling during fasting can therefore be seen as a regulator of the immune system as it influences the release of inflammatory cytokines, such as IL-6, in the body [33,34,35]. Moreover, intermittent fasting can delay immune senescence, which is characterised by a progressive decline in immune function with increasing age, according to a publication in which the number of hematopoietic stem cells increased fivefold through a fast-imitating diet [36]. Further major changes as a result of nutrition restriction and lowered insulin levels in metabolic pathways and cellular processes, such as lipolysis, autophagy, and increased lifespan, have been discussed in previous reviews [1,37]. Thus, a metabolic change caused by fasting can potentially be as medically effective as approved drugs [38,39,40].
Although the application of meal replacement is still a controversial topic, previous work [12,41] and reviews concerning such intervention studies have shown that adding meal replacement to lifestyle interventions can lead to greater weight reductions [42]. Since it has been shown that an effective change in lifestyle and diet can only be successful in the long-term with intensive support [43], an intervention should be started with high-protein, low-glycaemic meal replacement for the diet change. The advantage here is that the meal composition is clear and easy to use while also containing all the necessary nutrients, vitamins, minerals, and trace elements. In addition, it has been shown that meal replacement can actively reduce insulin levels and these effects can be already seen after one week. Through meal replacement the daily insulin demand could be reduced by 40% in insulin-treated type-2-diabetes patients [44], while in noninsulin-treated type-2-diabetes patients fasting insulin levels reduced by more than half [11]. Concomitantly, Lim et al. [11] demonstrated that the inhibited second-phase insulin secretion is restored after a successful meal replacement-based intervention, indicating that carbohydrate restriction by meal replacement is able to return insulin secretion back to physiological levels. Similar fast effects could only be seen after Roux-en-Y gastric bypass surgery where diabetes remission was accompanied by the normalisation of fasting insulin levels within a few days before significant weight loss occurred and although patients were still obese [45].
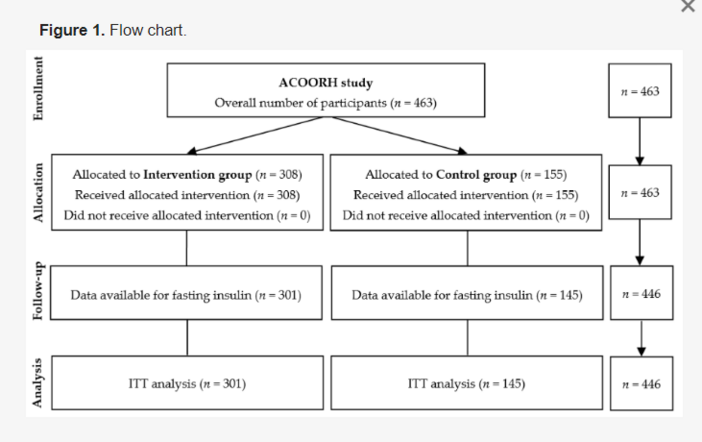
If only the ITT analysis is considered, the present data must be viewed with reservations. Since it contains the data of the participants who adhered to the study protocol, as well as those who already finished the meal replacement after four weeks, there is the possibility of an underestimation of the results. The actual effects are therefore better reflected by the completers analysis, as it shows which effects can be achieved when the meal replacement is applied according to the study protocol. The following also applies in any study: those who do not change their lifestyle cannot expect any improvement in metabolic values. However, the data show that even a four-week use of a meal replacement leads to a weight loss comparable to that achieved by the completers of the control group.
A further limitation of the study is that after six months the participants were no longer intensively supported. By stopping the meal replacement and returning to normal eating habits with meals composed of 20 g/day higher carbohydrate content than the meal replacement (carbohydrate consumption in the intervention group was 198 ± 71 g/day at baseline, 146 ± 83 g/day after 12 weeks and 170 ± 95 after 52 weeks [14]) an increase in insulin levels was observed, which in turn was associated with a weight re-gain of approximately 1 kg over six months. Prospectively, the increasing carbohydrate consumption and a subsequent weight gain might support a re-alteration of energy production in immune cells, i.e., from fat oxidation to glycolysis. Consequently, this might lead to a re-increase in inflammation markers and would confirm the regulatory role of insulin in subclinical inflammation. In further studies it would therefore be interesting to examine the effect of re-increasing carbohydrate consumption on the course of CRP and IL-6 and other inflammatory markers.