Discussion
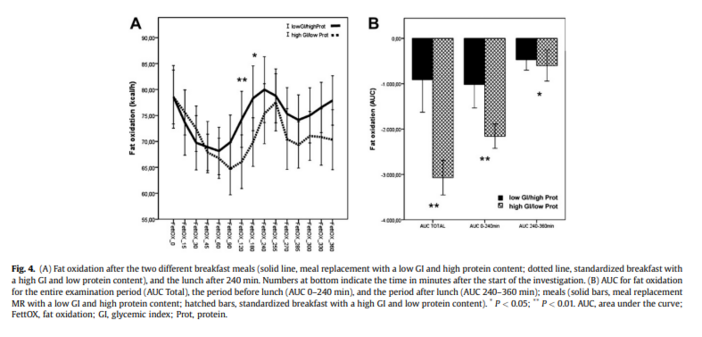
The most important finding of the present investigation was that, in obese insulin-resistant subjects, fat oxidation was significantly higher after the intake of an MR with a low GI and high soy protein content compared with an SB with a high GI and low protein content. This effect was also detectable after lunch in terms of a second meal effect.
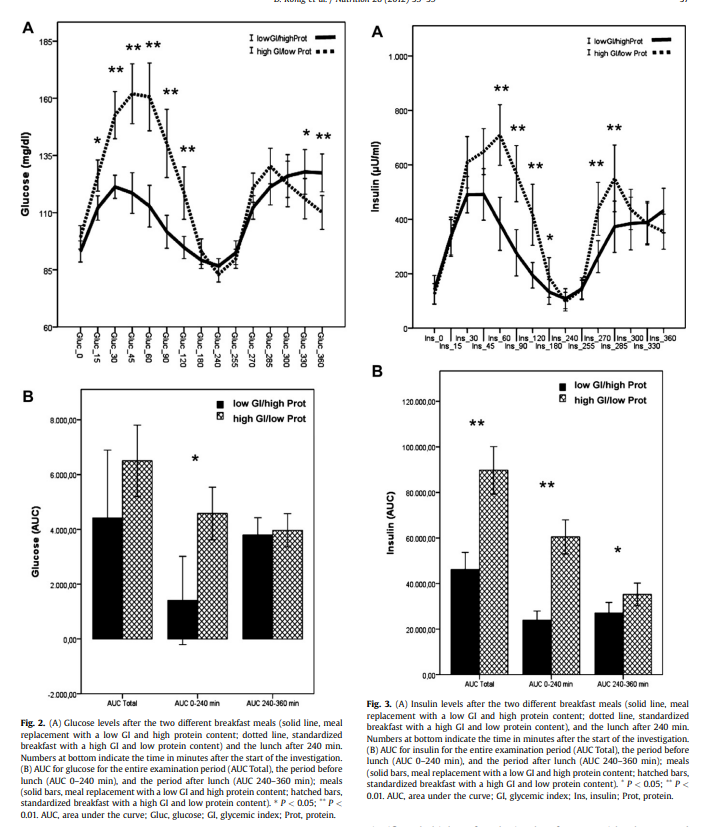
From the difference in glucose and insulin levels depending on the type of breakfast, it is very likely that the lower insulin concentrations are responsible for the higher fat oxidation after the MR [20]. It has been speculated that fat transport across the cell membrane is increased and fat oxidation is decreased in obese subjects and particularly in those with the metabolic syndrome [21,22]. Although the hypothesis is not supported by all findings, there is evidence that the decreased fat oxidation is responsible for intracellular fat accumulation, lipo-toxicity, and eventually for insulin resistance [12,14,23–25]. Therefore, it could be speculated that the increased fat oxidation after the intake of an MR could account not only for better weight loss but also for the observed rapid improvement in metabolic risk factors [7,26].
In addition, the results demonstrate that in insulin-resistant subjects, the amount of fat oxidation can be influenced by the GI and insulinemic index of a meal. Although the role and importance of the GI in daily nutrition is still under debate, more studies have demonstrated its role in the pathogenesis and prevalence of the metabolic syndrome [11]. The low GI and insulinemic index of the MR (soy–yogurt–honey preparation) is mainly determined by the amino acid pattern, but the isoflavones genistein and daidzein have also been shown to contribute to the lower pancreatic insulin secretion and the lower expression of transcription factors associated with lipo-toxicity such as sterol regulatory element binding protein-1 [21,27].
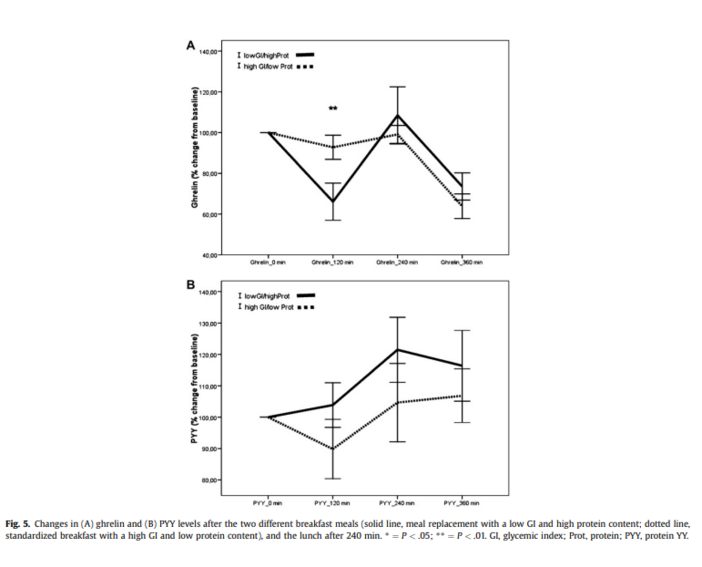
Another important aspect that has been described by some investigators concerns the greater and longer satiety after the intake of a protein-based MR with a low GI [17]. We found that ghrelin concentrations were significantly lower 2 h after intake of the MR compared with the SB. After lunch, the decrease in ghrelin levels was almost identical. The reason for the greater decrease in ghrelin after the MR cannot be answered conclusively. In some investigations, ghrelin levels have been correlated with insulin levels, whereas others could not establish such a relation [28]. Data regarding how far the amino acid composition could have influenced the postprandial course of ghrelin and PYY are still lacking. Nevertheless, the significantly greater decrease in ghrelin levels and the trend toward higher PYY concentrations in the postprandial period likely contribute to the greater and longer satiety found after the intake of MRs [17].
It should be mentioned, however, that the number of subjects investigated was rather small. The results need to be reproduced in a larger cohort and in subjects differing in age, body mass index, and gender.
In conclusion, compared with the high GI/low protein SB, a high soy protein MR with a low GI was associated with lower glycemia and insulinemia and a relatively higher fat oxidation in the postprandial period. Together with a favorable course of appetite-regulating hormones, this could further explain the success of this MR regimine for weight reduction and improvement of metabolic risk factors.